Responsible: Dott.ssa M.G. D'Angelo e Dott.ssa F. Magri
Collaborative work between IRCCS E. Medea di Bosisio Parini and Fondazione Policlinico di Milano- Clinica
In recent years, muscle magnetic resonance imaging (MRI) has played an increasingly important role both in diagnostics and in the evaluation of therapeutic efficacy in neuromuscular and neuromotor pathologies.
In muscle diseases, the study of muscle MRI can, through the identification of specific patterns of muscle involvement, guide towards a more immediate differential diagnosis in the genetic and biochemical fields. Furthermore, the specific study of respiratory muscles and its correlation with functional parameters can provide useful tools for predictive purposes or for evaluating the effectiveness of certain treatments (R-Y Carlier, 2012; Hollingworth KG, 2012).
In particular, muscle MRI has been the subject of numerous studies, especially in recent years.
Recent work, mainly carried out with 1.5T MRI (Hollingsworth KG et al 2012, Astrea G 2009, Astrea G 2012), has allowed the definition of specific patterns of muscle involvement in different forms of muscular dystrophy suggesting the possible application of this tool to guide differential diagnosis. At present, most of the work has investigated lower limb involvement, although some whole body MRI studies have been published (Kesper K et al., 2008).
Furthermore, few longitudinal studies have been conducted so far (Willis TA et al. 2013) The acquisition of longitudinal data could instead be crucial in order to evaluate the effectiveness of this tool to trace the natural history of disease and as an outcome measure in the evaluation of efficacy in potential future pharmacological studies.
- The Study
- Background
- Objectives
- Sample
- Activity Consent
- Activities Characterization
- Imaging Activities
- Preliminary Data
The study aims to select 20 patients with Muscular Dystrophy of the Crawlers (divided by type on the basis of the gene involved), 5 patients with Congenital Myopathy and 5 patients with Congenital Dystrophy. Our purpose is to study patients affected by muscular dystrophy at time 0 and at subsequent times at 12 and 24 months distance.
3 T acquisitions of the scapular girdle and proximal upper limb musculature will be performed, using T1, T2, inversion recovery and 3 point Dixon weighted sequences (Hollingsworth KG et al 2012, Astrea G 2009, Astrea G 2012). The degree of muscle involvement will be assessed with semi-quantitative criteria using specific scales (Mercuri E. et al, 2002). In a subgroup of patients will also be used specific sequences able to assess muscle perfusion, in order to define the presence of an impairment of perfusion and metabolic impairment in some types of muscle diseases studied.
In a limited subgroup of patients we will also conduct an exploratory study in order to go to evaluate the sensitivity and specificity of the MRI study of intercostal, abdominal and diaphragmatic muscles and any correlation with respiratory function.
In the group of subjects affected instead by neuromotor pathologies such as hereditary spastic paraparesis and infantile cerebral palsy, we aim to define the morphology of a muscle etiopathogenically intact from a structural point of view but subjected to stress of "central" origin and to define the role on it of local myorelaxant treatments such as botulinum toxin and possibly identify modulating agents of different effectiveness.
We will study by muscle MRI (assuming study of gastrocnemius muscle and quadriceps femoris) 5 subjects with hereditary spastic paraparesis (HSP) and 5 subjects with PCI never treated with botulinum toxin and respectively 5 subjects HSP and 5 PCI subjects already previously treated, pre and post treatment with botulinum toxin.
Neuromuscular diseases are a clinically and genetically heterogeneous group of diseases characterized by progressive and progressive muscle weakness often associated with cardiac, respiratory and cognitive involvement. Currently there are no effective therapies and more than 50% of these forms are still without a molecular diagnosis, due to the complexity of the diagnostic process. However, a correct definition of the molecular basis is an essential prerequisite for clinical management, to further study the pathogenesis and to formulate therapeutic hypotheses.
Recently, the development of new diagnostic strategies such as genetic analysis by Next-generation Sequencing or the application of muscle MRI have refined the diagnostic capability for this group of diseases, leading to interesting results and a better understanding of the pathogenesis, although both of the mentioned techniques are not yet routinely applied.
Main Objective
The main objective of the study is to improve the diagnostic process of some of the main forms of neuromuscular diseases and to investigate their pathogenetic mechanisms. The study by muscle MRI is mainly aimed at identifying specific patterns of muscle involvement that can be used to guide the differential diagnosis and the evolution of the disease. The study by MRI of respiratory muscles and its correlation with functional parameters may provide useful tools for predictive purposes or to assess the function of the different diseases in different stages of progression.
Secondary Objective
Longitudinal evaluation of a group of genetically defined patients with cingulate dystrophy. Motor function assessments with internationally recognized scales (Motor Function Measure scale) and 6 minute walk test (in patients still ambulatory) and muscle strength assessments using MRC scale will be compared to imaging data obtained. The usefulness of muscle imaging in the follow-up of the different forms and as a potential clinical out for future therapeutic trials, in possible replacement of muscle biopsy, will be evaluated.
The present study is an exploratory study, aimed at defining the role and sensitivity of MRI in assessing the degree of skeletal and respiratory muscle involvement in subjects with primary and secondary muscle suffering. To date, the studies carried out and published in the literature are based on small samples of patients.
An overall sample of 50 subjects will be studied, subdivided in turn into different groups according to the pathology considered. On the whole, for each type of pathology at least 5 patients with different degrees of muscular impairment will be evaluated. We believe that this number of patients is sufficient to allow a comparative study and to define any differences between the subgroups studied. On the basis of the results obtained it may be decided to further expand the sample size.
Acquisition of informed consent
In this first year we proceeded, after the collection of Informed Consent, with the clinical characterization of patients through:
- collection of anamnestic data and data related to the presence of any familiarity and data related to the diagnosis including data of genetic analysis, biochemical and muscular histology.
- detailed neurological evaluation carried out by means of strength measurements (MRC scale) and execution of functional scales such as the Motor Function Measure (MFM) scale and the 6 minute walk test (carried out in patients who are still ambulatory) and, where possible, also the functionality of the upper limbs through the Upper Limb scale.
All patients also underwent :
- evaluation of respiratory function (by spirometry, nocturnal saturimetry recording, and optoelectronic plethysmography) and cardiac function (by echocardiogram, electrocardiogram-ECG and, where necessary, ECG-holter recording).
Clinical characterization of patients
All data are entered in a computerized DATABASE system (whose creation was made possible thanks to a Current Research project of the past years), with password-restricted access; the "neuromuscular database" is a web application designed to collect and report the collected data of patients affected by neuromuscular pathologies.
The software was developed with PHP language, using the "RadPHP" framework, while the data is stored in the relational database PostgreSQL; both the PHP application and the database engine are hosted in the Linux sever. The use of standard Html, Css and Javascript technologies to create the user interface makes the application accessible to all users with a Web browsing system, without the need for a local installation of other applications.
Thanks to this Web-based approach, access to the system is not limited to the computer stations of our Structure but can be managed on PCs outside the Institute, with the aim of facilitating the collection of data on the same patient from different health facilities.
There is a system for tracking user access, with profile management; each user is associated with a specific profile that determines the accessibility of the various cards in read-only or write-only on the basis of professional skills and study protocols for which the database is used.
Finally, the personal data have been decoupled from clinical data to allow the anonymous processing of personal data of patients for processing and statistical analysis.
Data can be aggregated and filtered with the aim of obtaining information on a single patient (e.g. to evaluate the evolution of some parameters in a single subject) or on a group of patients. The results can be easily saved and imported to an Excel file (or other spreadsheets) or to statistical analysis systems such as SPSS, where the user can use the information to create graphs or statistical analysis.
Below are some examples: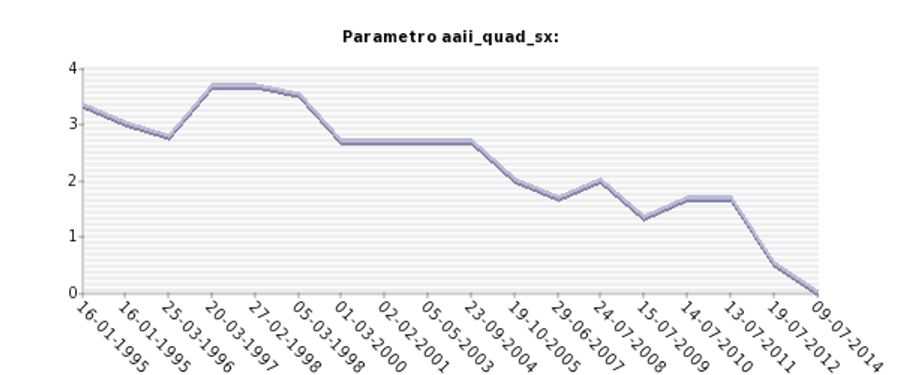
Graph obtained from the database: Longitudinal analysis of left quadriceps femoris muscle fatigue, measured by MRC scale (0-5) in a patient with calpain-deficient muscular dystrophy of the belts 3
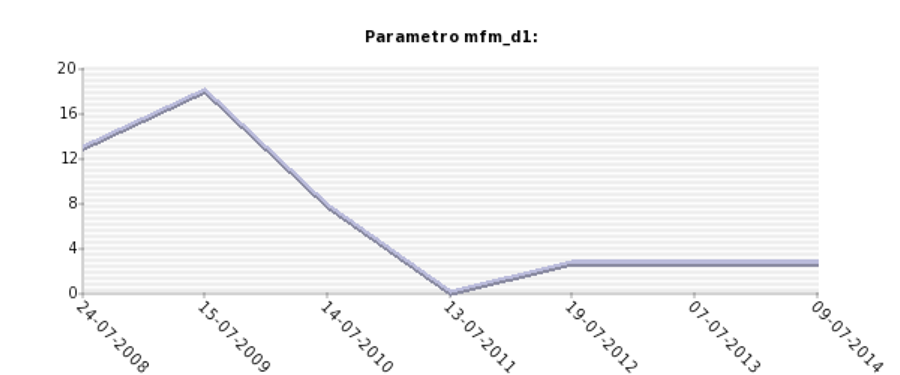
Graph obtained from the database: Longitudinal analysis of the Motor Function Measure scale, subscale D1 (standing/transferring), measured using the MRC scale (0-5) in a patient with calpain-deficient muscular dystrophy of the belts 3
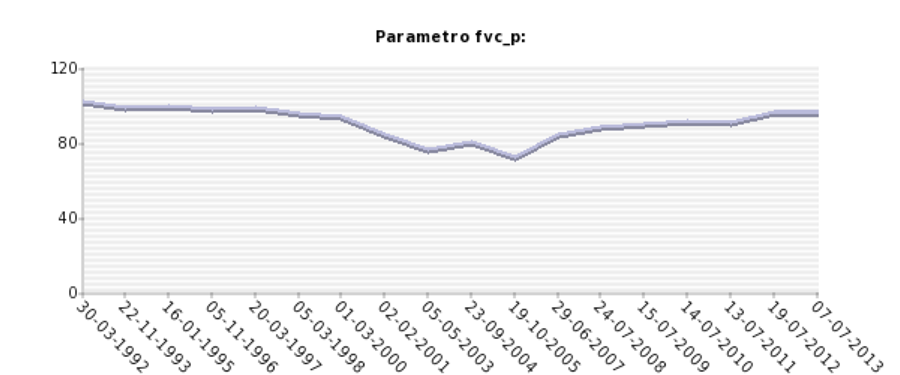
Graph obtained from the database: Longitudinal analysis of functional motor assessment by spirometry (FVC parameter) in a patient with calpain-deficient muscular dystrophy of the cingulate 3
Thanks to the clinical data collected, we started an analysis aimed at identifying both in each individual subject and in the group to which the individual belongs (e.g. calpain 3-LGMD2A deficiency muscular dystrophy group).
Evaluating the data obtained on the muscle scales (MRC), we identified the muscle(s) most severely affected by the evolution of the disease, those least affected, and the role played by the duration of the disease on the evolution/non-evolution of the hyposthenic picture.
The observations of the motor function data, collected by means of the MFM scale (Motor Function Measure, internationally validated), show how the value obtained at the D1 subscale (orthostatism and transfers) is absolutely the most suggestive of the motor condition of a patient affected by calpain-deficient muscular dystrophy3. In fact, a value of D1 < 12 corresponds to a loss of walking in all subjects, while a value between 40 and 60 of the total score of the scale is associated with an important clinical and functional variability, including patients with independent walking and patients confined to a wheelchair.
These preliminary observations may be valuable for subsequent observations/corrections of muscle imaging data.
Muscle Imaging Data Collection
In all patients 3T acquisitions of the scapular girdle muscles and the proximal muscles of the upper and lower limbs will be performed, using T1, T2, inversion recovery, 3 point Dixon weighted sequences as previously described (Hollingsworth KG et al 2012, Astrea G 2009, Astrea G 2012). The degree of muscle involvement will be assessed with semi-quantitative criteria using previously published scales (Mercuri E. et al, 2002). The possibility, in a subgroup of patients, of applying quantitative parameters will also be evaluated. The study will be completed with muscle perfusion sequences.
In a limited subgroup of patients we will also conduct an exploratory study in order to evaluate the sensitivity and specificity of the MRI study of respiratory muscles (intercostal muscles, abdominal muscles and diaphragm) and the possible correlation with respiratory function measured by spirometry and optoelectronic plethysmography.
During 2015, the first MRI studies were performed on patients with muscular dystrophy of both known/genetically determined etiology and genetic etiology not yet defined.
The MRI protocol optimized ad hoc for the study included sequences:
- T1-weighted for morphological characterization of muscle
- T2-weighted multi-echo for quantification of tissue T2 parameter
- DIXON for signal separation of water and fat, with quantification of fat fraction.
- Diffusion MR spinEcho at multiple b-values, for structural analysis of muscle tissue, by quantification of FA (fractional anisotropy) parameter and tractographic reconstructions (DTI).
7 healthy subjects and 22 patients with different forms of muscular dystrophy (8 calpain deficiency, 3 dysferlin deficiency, 4 Becker's dystrophies, 1 anoctamine deficiency, 1 β-sarcoglycan deficiency, 1 collagen type VI deficiency, 1 facio-scapulo-humeral dystrophy, 3 patients with ndd cingulate dystrophy) underwent muscle MRI.
The examinations were acquired with a 3T MRI scanner and the thigh muscles were investigated. All subjects tolerated the examination and no complications occurred while performing the MRI investigations.
Data from each subject were processed to obtain structural maps, T2 parameter maps, FA maps and fat-fraction (FF) maps.
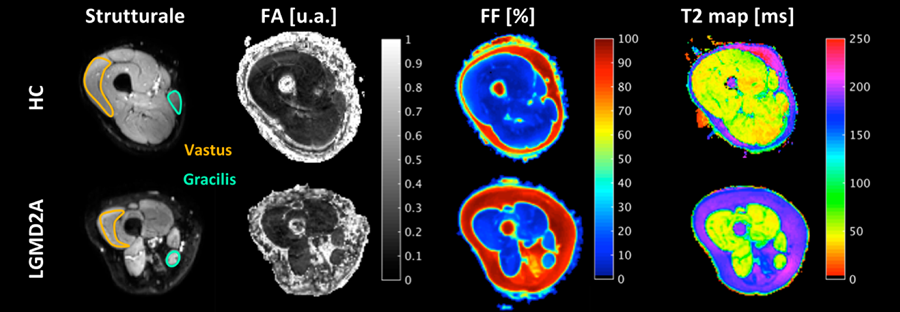
In the sample of healthy people, the measurements carried out showed homogeneity and inter-subject repeatability for all the variables considered so far (FA, T2, FF).
In the group of patients, these variables proved to be sensitive in measuring the architectural and structural modifications of the muscle. In particular, preliminary measurements were carried out at the level of the vastus medialis and gracilis muscles which showed different behaviours and modifications of the parameters considered in relation to the state of structural alteration and the muscle group considered.
The feasibility of tractographic reconstructions at the level of both healthy and pathological muscle tissue has also been demonstrated, with evidence of the architectural subversion of muscle fibers in patients affected by different forms of dystrophy.
CONCLUSIONS
The aim of this study was to apply quantitative MRI (qMRI) to assess structural modifications in thigh muscles of subjects with limb girdle muscular dystrophy (LGMD) 2A and 2B with long disease duration. Methods: Eleven LGMD2A, 9 LGMD2B patients and 11 healthy controls underwent a multiparametric 3T MRI examination of the thigh. The protocol included structural T1weighted images, DIXON sequences for fat fraction calculation, T2 values quantification and diffusion MRI. Region of interest analysis was performed on 4 different compartments (anterior compartment, posterior compartment, gracilis, sartorius). Results: Patients showed high levels of fat infiltration as measured by DIXON sequences. Sartorius and anterior compartment were more infiltrated in LGMD2B than LGMD2A patients. T2 values were mildly reduced in both disorders. Correlations between clinical scores and qMRI were found. Conclu- sions: qMRI measures may help to quantify muscular degeneration, but careful interpretation is needed when fat infiltration is massive.
 Download the Fulltext in English
Download the Fulltext in English